Mohs Surgery Compared to Traditional Excision

Mohs surgery and traditional excision are both used to treat skin cancer, but they differ in how cancer is removed and evaluated. This page explains the key differences between these approaches, including when each may be recommended and how treatment decisions are made.
When deciding how to treat skin cancer, patients are often presented with more than one surgical option. Mohs surgery and traditional surgical excision are both widely used, evidence-based treatments, but they differ in how the cancer is removed and evaluated. Understanding these differences can help patients feel more informed and confident as they discuss treatment recommendations with their dermatologist or surgeon.
Understanding Skin Cancer Surgery Options
Several surgical approaches are used to remove skin cancer. Mohs surgery and traditional excision are among the most common options, and each has specific indications based on the type, size, and location of the cancer.
Overview of Mohs Surgery
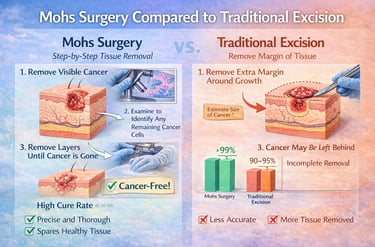
Mohs surgery is a specialized form of dermatologic surgery that removes skin cancer in thin layers. Each layer is examined under a microscope during the procedure to determine whether cancer cells remain.
This process continues until no cancer cells are detected. By evaluating the entire surgical margin, Mohs surgery allows for precise cancer removal while preserving as much healthy skin as possible.
Overview of Traditional Excision
Traditional excision involves removing the visible tumor along with a predetermined margin of surrounding healthy skin. The wound is typically closed at the time of surgery.
The removed tissue is sent to a laboratory for analysis, where a portion of the margins is examined days later. Traditional excision is an effective and commonly used treatment for many low-risk skin cancers.
How Mohs Surgery and Traditional Excision Differ
While both Mohs surgery and traditional excision are effective surgical treatments for skin cancer, they differ in how cancer margins are evaluated and how much healthy tissue is removed. These differences can influence treatment recommendations, especially for cancers in sensitive or high-risk areas.
Margin Evaluation Methods
A key difference between the two procedures is how the edges, or margins, of the removed tissue are examined.
With Mohs surgery, nearly 100% of the surgical margins are examined under a microscope during the procedure. This allows the surgeon to confirm complete cancer removal before reconstruction.
With traditional excision, the removed tissue is sent to a laboratory, where only selected sections of the margins are examined. Results are typically available days later, and additional treatment may be needed if cancer cells are found at the edges.
Tissue Preservation
Mohs surgery is designed to remove only tissue that contains cancer. By targeting cancer cells precisely, the procedure preserves as much healthy skin as possible.
Traditional excision removes the tumor along with a standard margin of surrounding skin. While this approach is effective for many low-risk cancers, it may remove more healthy tissue than necessary, particularly in areas where tissue conservation is important.
Accuracy & Cure Rates
Both Mohs surgery and traditional excision are effective treatments for skin cancer, but they differ in accuracy and long-term cure rates. These differences are largely related to how completely cancer margins are evaluated during each procedure.
Cure Rates with Mohs Surgery
Mohs surgery is known for its high accuracy and strong long-term cure rates. By examining nearly all of the surgical margins during the procedure, Mohs surgery allows for precise identification and removal of cancer cells.
For appropriately selected cases, reported cure rates for Mohs surgery are up to 99% for primary basal cell carcinoma and approximately 97–98% for primary squamous cell carcinoma. Cure rates remain high even for recurrent or higher-risk tumors.
Cure Rates with Traditional Excision
Traditional excision also offers good outcomes for many skin cancers, particularly low-risk tumors. Cure rates vary depending on tumor type, location, and margin size.
For primary basal cell and squamous cell carcinomas treated with standard excision, reported cure rates are generally around 90–95%. While effective in many cases, traditional excision has higher recurrence rates compared to Mohs surgery for certain high-risk or recurrent skin cancers.
As with all treatments, cure rates represent overall trends and do not guarantee individual outcomes.
When Mohs Surgery Is Preferred
Mohs surgery is not necessary for every skin cancer. It is typically recommended when specific features increase the risk of recurrence or when preserving healthy tissue is especially important. In these situations, the precision of Mohs surgery offers clear advantages.
High-Risk or Recurrent Skin Cancers
Mohs surgery is often preferred for skin cancers considered high-risk or those that have returned after previous treatment. These cancers may grow in less predictable patterns and be more difficult to remove completely.
Mohs surgery may be recommended when a skin cancer:
Has recurred after prior treatment
Has aggressive or poorly defined borders
Is large or growing quickly
Shows features associated with higher recurrence risk
The ability to track and remove cancer cells precisely makes Mohs surgery especially valuable in these cases.
Cancers in Sensitive or Visible Areas
Skin cancers located in areas where function and appearance are critical often benefit from the tissue-sparing approach of Mohs surgery. Common locations include the face, ears, eyelids, nose, lips, hands, and feet.
In these areas, Mohs surgery helps:
Preserve normal movement and sensation
Maintain natural contours and symmetry
Minimize removal of healthy skin
This balance of accuracy and tissue preservation is a key reason Mohs surgery is frequently recommended for visible or anatomically complex areas.
When Traditional Excision May Be Appropriate
Traditional surgical excision remains an effective and appropriate treatment option for many patients with skin cancer. The choice of procedure depends on tumor characteristics, location, and overall risk profile.
Low-Risk Skin Cancers
Traditional excision is often suitable for skin cancers that are considered low risk. These cancers are typically small, well-defined, and have not been treated before.
Low-risk features may include:
Primary (first-time) tumors
Well-defined borders
Slow-growing behavior
Locations outside high-risk cosmetic or functional areas
In these cases, traditional excision can provide reliable cancer removal with good outcomes.
Simpler Surgical Situations
Traditional excision may also be appropriate when the surgical site is straightforward and tissue preservation is less critical. Areas with more available skin may allow for standard margins and uncomplicated closure.
For many patients, traditional excision offers:
A single-stage procedure
Predictable healing
Effective treatment for appropriately selected cancers
Your dermatologist will recommend the most appropriate surgical approach based on established medical guidelines and your specific diagnosis.
Surgical Process & Timing
Mohs surgery and traditional excision differ not only in technique, but also in how and when results are confirmed. Understanding these timing differences can help patients know what to expect on the day of surgery and afterward.
Same-Day Results with Mohs Surgery
Mohs surgery is performed in stages, with tissue examined during the procedure. After each layer is removed, it is processed and reviewed under a microscope on the same day.
This approach allows the surgeon to:
Identify and remove remaining cancer immediately
Confirm clear margins before reconstruction
Complete treatment in a single visit in most cases
Patients typically wait comfortably between stages while tissue is analyzed.
Pathology Timing with Traditional Excision
With traditional excision, the tumor and surrounding margin are removed and the wound is closed during the procedure. The tissue is then sent to an external pathology laboratory.
Pathology results are usually available several days later. If cancer cells are found at the margins, additional treatment or another surgery may be needed. This delayed margin assessment is a key difference between traditional excision and Mohs surgery.
Scarring & Cosmetic Outcomes
Scarring is a natural part of any skin surgery. The size and appearance of a scar can vary depending on the surgical technique, the location of the cancer, and how the skin heals over time.
Tissue Preservation & Cosmetic Results
Mohs surgery is designed to preserve as much healthy skin as possible. By removing only tissue that contains cancer, the final surgical wound is often smaller than it would be with other techniques.
Preserving surrounding skin can help:
Maintain natural contours
Reduce tension on the wound
Support more refined reconstruction
This tissue-sparing approach often contributes to favorable cosmetic results, especially in visible areas.
Scar Size & Appearance Differences
Traditional excision removes the cancer along with a standard margin of surrounding skin, which may result in a larger surgical site. In many cases, this heals well, particularly in areas with more available skin.
With Mohs surgery, scars may be smaller due to more precise removal. Regardless of the technique used, scars typically continue to improve in appearance over several months, and proper wound care plays an important role in healing.
Recovery & Follow-Up Differences
Recovery and follow-up care are important parts of any skin cancer treatment. While healing experiences vary, Mohs surgery and traditional excision have some differences in how recovery and post-treatment monitoring are managed.
Recovery After Mohs Surgery
Most patients go home the same day after Mohs surgery. Because cancer removal and margin evaluation are completed during the procedure, additional surgery is usually not needed at the treated site.
Recovery after Mohs surgery may include:
Mild swelling, bruising, or tenderness for several days
Stitches that are removed within 1–2 weeks, depending on location
Detailed wound care instructions and a scheduled follow-up visit
Patients are typically advised to limit strenuous activity during early healing and to continue routine skin examinations long term.
Recovery After Traditional Excision
Recovery after traditional excision is often straightforward, especially for smaller or low-risk tumors. The wound is closed at the time of surgery, and patients usually resume normal activities within a short period.
However, because pathology results are delayed, follow-up may include:
Reviewing pathology findings several days later
Additional treatment if cancer cells are found at the margins
Routine wound checks and suture removal
Both procedures require ongoing skin monitoring, as having one skin cancer increases the risk of developing others in the future.
How Your Dermatologist Chooses the Best Approach
Selecting the most appropriate treatment for skin cancer involves careful medical judgment. Dermatologists consider both tumor-related details and individual patient factors to determine whether Mohs surgery or traditional excision is the best option.
Tumor Characteristics
The features of the skin cancer itself play a major role in treatment selection. Certain characteristics increase the need for precise margin control and tissue preservation.
Tumor-related factors may include:
Type of skin cancer
Size and depth of the tumor
Location on the body
Border definition and growth pattern
Whether the cancer is primary or recurrent
High-risk features often favor Mohs surgery, while lower-risk tumors may be well suited to traditional excision.
Patient-Specific Factors
Individual health and lifestyle considerations are also important when planning treatment. These factors help ensure that care is safe, appropriate, and tailored to the patient.
Patient-specific factors may include:
Age and overall health
Immune system status
Prior skin cancer history
Ability to attend follow-up visits
Personal preferences after discussing options
Your dermatologist will review these factors with you and explain the reasoning behind their recommendation, helping you make an informed decision about your care.
Frequently Asked Questions About Mohs vs Traditional Excision
Patients often have questions about how Mohs surgery compares with traditional excision and why one approach may be recommended over another. The answers below provide general information to help clarify common concerns.
Common Comparison Questions
Is Mohs surgery better than traditional excision?
Neither procedure is universally “better.” Mohs surgery offers higher cure rates and greater tissue preservation for certain high-risk or sensitive cases, while traditional excision is effective for many low-risk skin cancers.
Why wasn’t Mohs surgery recommended for my skin cancer?
Not all skin cancers require the level of precision provided by Mohs surgery. For small, low-risk tumors in less sensitive areas, traditional excision may be an appropriate and effective option.
Does Mohs surgery take longer than traditional excision?
Mohs surgery often takes more time on the day of treatment because tissue is examined during the procedure. Traditional excision is usually faster, but may require additional treatment if margins are not clear.
Do both procedures leave scars?
Yes. Any surgical procedure will result in a scar. The size and appearance depend on the technique used, the location of the surgery, and how the skin heals over time.
Will I need additional treatment after either procedure?
Most patients do not need further treatment after successful surgery. However, if cancer cells are found at the margins after traditional excision, additional treatment may be required.


Request a Mohs Consultation
Copyright © 2026 | Savannah Mohs Surgery | All Rights Reserved.
Privacy Policy | Terms and Conditions | Accessibility
Monday: 8:00am - 5:00pm
Tuesday: 8:00am - 5:00pm
Wednesday: 8:00am - 5:00pm
Thursday: 8:00am - 5:00pm
Friday: 8:00am - 5:00pm
Office Hours
Learn More
Reach Out
Resources
Address
Request Consultation
Call Now
(704) 858-6585
Savannah Mohs Surgery
Serving Savannah, GA and Surrounding areas.

